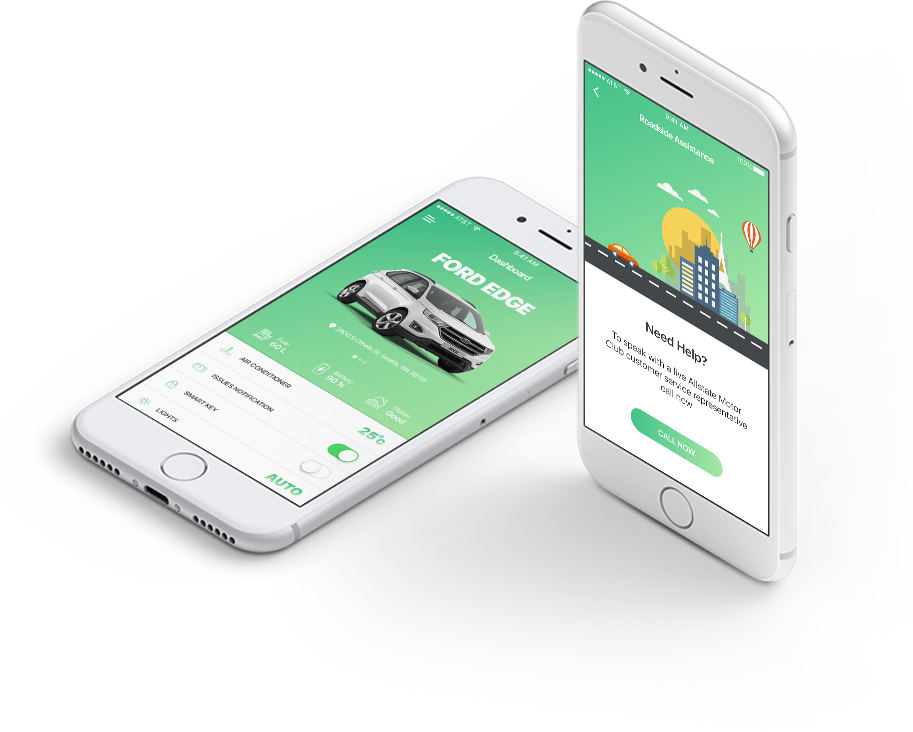
24/7 Support
Our team is available 24/7, ensuring you never have to wait for assistance when you need it most.
With powerful features and a user-friendly design, our app helps
you stay organized, efficient, and in control.
Our team is available 24/7, ensuring you never have to wait for assistance when you need it most.
We’re committed to safeguarding your personal information and ensuring it’s handled with complete confidentiality.
Our code is designed with simplicity and readability in mind, making it easy for developers to understand and maintain.

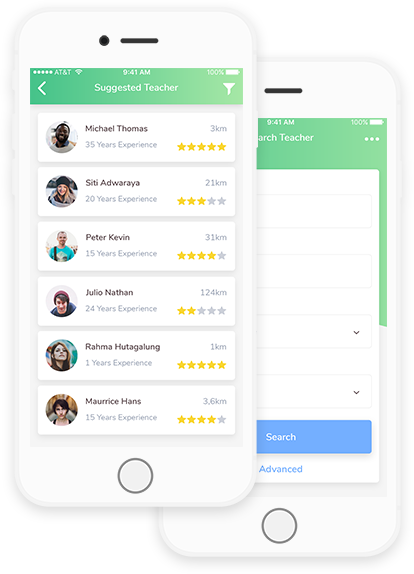
Intuitive interface for a seamless experience.

Crisp, clean text for enhanced readability.

Lightning-quick performance with minimal lag.

A visually appealing, modern aesthetic.

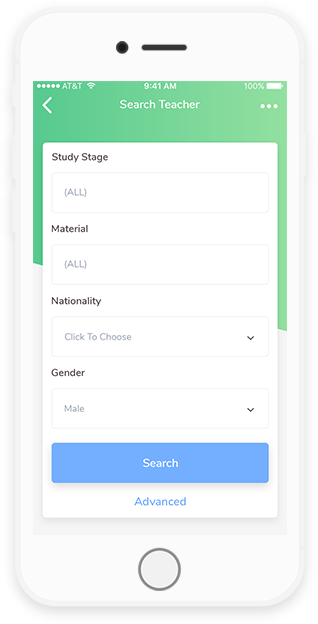
Access a wide range of powerful tools and options.

Quick setup with minimal effort required.

Comprehensive guides and resources for easy navigation.

Optimized for peak performance and speed.
Many devices also come with built-in screenshot features, allowing users to easily capture
and save images of their screens for later reference or sharing.



Most such devices are sold with several apps bundled as pre-installed software,
such as a web browser, email client, calendar, mapping program.
We're here to help! Whether you have a question, feedback, or need support, feel free to reach out to our team. Get in touch with us
through the contact form, email, or phone, and we'll respond as quickly as possible.